

Abstract
BACKGROUND: Warfarin is one of the most widely used anticoagulation medications. It requires frequent monitoring due to its chemical and physiological nature. A majority of patients need to maintain an INR between 2.0 and 3.0. Previous research has shown that patients who can maintain a higher time in therapeutic range (TTR) have improved outcomes. For some patients, this can be difficult to achieve. Clinicians utilize numerous strategies to improve TTR in their patients. The diversity of methods, disparate outcomes, and varying levels of evidence means that researchers and clinicians are often overwhelmed by the comparisons.
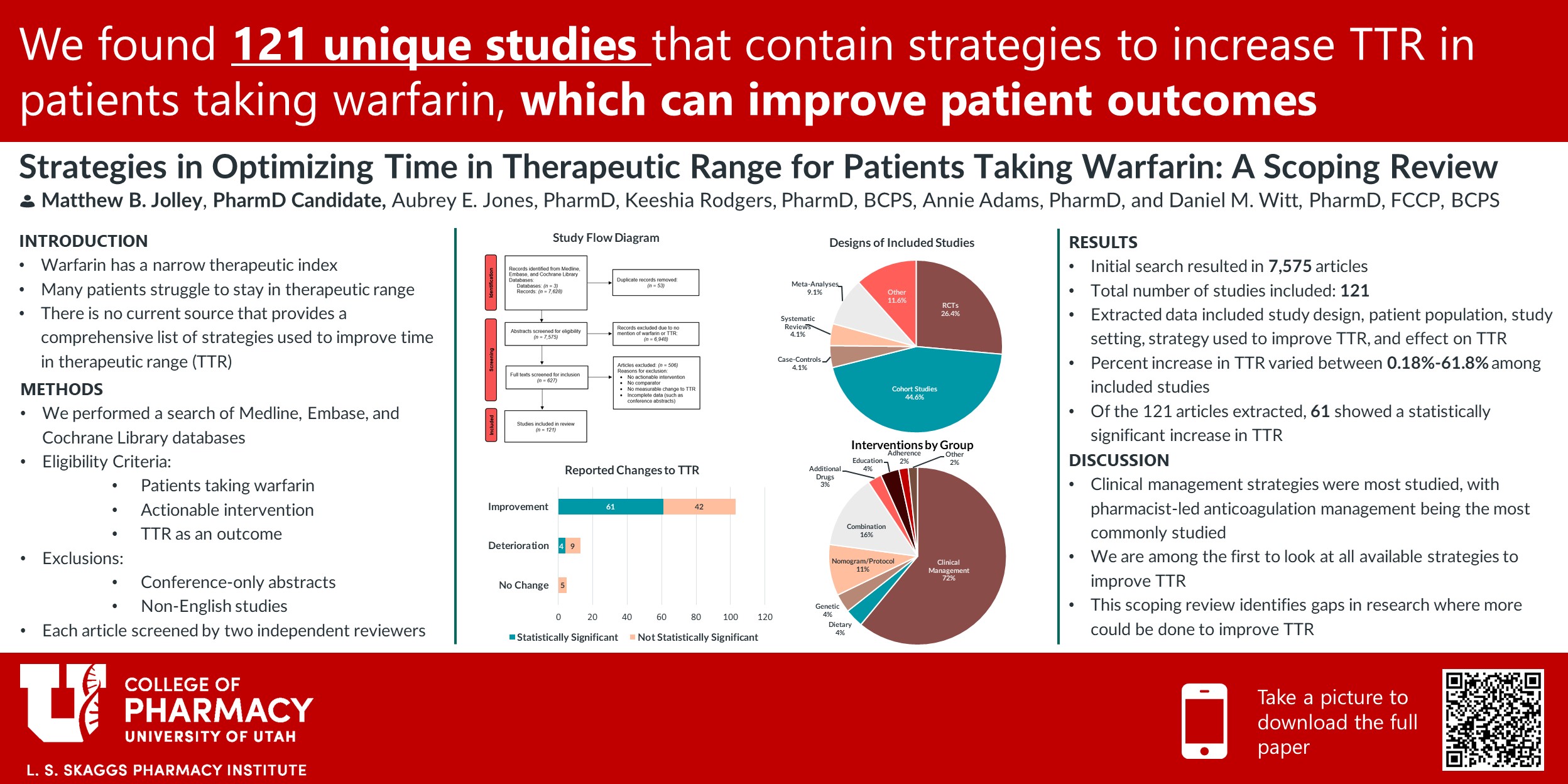
OBJECTIVE: Our objective is to gather all known strategies used to optimize TTR in warfarin patients and provide a resource that clinicians can use to improve patient outcomes. We also hope to identify any potential gaps in the literature so other studies may be done.
METHODS: We performed a scoping review, searching for articles in Medline, Embase, and Cochrane library databases including CENTRAL and International Pharmaceutical Abstracts. We searched for all articles that contained a combination of keywords and database subject terms for the drug “warfarin” and “time in therapeutic range” concepts.
RESULTS: An initial search result of 7,628 articles was reduced to 236 articles which underwent data extraction. Of the different strategies to improve TTR, a majority of the articles focused on clinical management (n=84, 69.4%), such as pharmacist managed anticoagulation. Other groups that contained a large number of strategies include strategies involving nomograms/protocols (n=27, 22.3%), pharmacogenetics (n=13, 10.7%, dietary factors (n=5, 4.1%), a combination of the groups previously mentioned (n=19, 15.7%), or others (n=10, 8.3%). These strategies offered varying degrees of improvement in TTR, with n=65, (53.7%) being statistically significant.
CONCLUSIONS: Our search provided numerous modalities in improving TTR in patients taking warfarin. Clinicians can use the results from our search to improve therapies for patients by applying strategies that show benefit in patients struggling to maintain within therapeutic range. Each patient’s situation is unique and may require a combination of strategies offered. By utilizing this resource, it is our hope that clinicians will be able to improve patient outcomes overall.

Responses
Matt – very good work!!. I would like to know more on the strategies described in the included studies. You mentioned 121 unique studies but I assume that the unique strategies might be fewer than that. How many unique strategies are out there. In particular, it would be great to know which strategies were effective based on previously conducted reviews or studies included. This may be beyond your scope and I think it is an ultimate goal for us to know that, right. Did you have a chance to review the strategies in 121 studies in details and provide a unique list?
Hi Nui! Thank you for your comment. You are correct, there were many studies that looked at similar things, but with some slight variations. For example, strategies related to vitamin k supplementation had varying amounts of vitamin k. Daily vitamin k supplementation ranged from 100 mcg daily to 200 mcg daily among included studies. So, while these studies were looking at the same thing (vitamin k supplementation to stabilize TTR), the differing doses being studied provided additional insight and variability. The question is, do we consider them all unique strategies because of the different doses? Or consider them the same since they are all vitamin k supplementation? We are actually still cleaning up the data, so I don’t have an official answer for you as to how many unique strategies there are yet, as we are still trying to answer that question. Also, due to so many studies being part of the Clinical Management group, we are hoping to break it up further into sub-groups like “Pharmacist-Driven Management” and “Patient Self-Management”. That will hopefully allow us to better understand how many truly unique strategies there are. Once that is completed we will be able to provide the list of all included studies.
We chose to include systematic reviews and meta-analyses on the subject as well, which meant that articles included in the meta-analyses were also likely included as separate articles. While we are still analyzing that data, we are hopeful that those reviews will at least provide additional insight and credibility into whatever strategy was being studied.
Great job, Matt. You really put a lot of effort into this study and I think it will be really helpful for providers trying to find ways to improve TTR. If you were to start working in an anticoagulation service, which of these interventions would be at the top of your list to try with a patient with suboptimal TTR? Why did you choose these interventions?
Hi Dan! Great question. If the clinician has not already done so, I would first consider adding a pharmacist to the management team, as that appears to have the most amount of data supporting that strategy. If they already have a pharmacist on board, I would then consider some type of patient self-testing or self-management to increase patient involvement and increase testing frequency. Third, I would maybe consider genetic testing, to better understand a patient’s warfarin metabolism profile. These recommendations are all based on the number of studies that appeared to show the greatest benefit with statistical significance. That being said, there are a number of other strategies that can be considered and each patient should be treated using the strategy that best meets their needs.
Important subject. Thank you.
Matt, I enjoyed reading your poster. Well done! In particular, I liked the logical development of the question, as well as the clear presentation of the results. The conclusions seem to flow logically from those results, as well! I’m curious as to whether there is something about the pharmacist-based management per se or whether it’s just greater management (typically provided by pharmacists) that leads to the better TTR?
Hi Dr. Keefe! Great question. I’m not entirely sure what explains it. The strategies that involved pharmacist-based management all had slight variations, such as a pharmacist calling and checking-in on the patient regularly, or having a pharmacist be the one to determine the patient’s dose following INR results. I could speculate that it may have to do with the fact that pharmacists are overall more familiar with medications in general and have a greater understanding of what affects warfarin concentrations, particularly in regards to drug-drug interactions and metabolism pathways. Regardless, I think this provides an opportunity for additional research to be done in order to better understand that!
Comments are closed.